
Two studies reported:
- Treatment for alcohol and opioid use disorders (AOUD) is feasible in primary care settings, but ongoing funding to support organizational capacity is critical for sustaining such programs.
- Specific patient characteristics influence what type of AOUD treatment primary care patients will initiate.
- A collaborative care model offering different therapeutic approaches may be an effective approach to AOUD treatment in primary care settings.
Many people with alcohol and opioid use disorders (AOUD) do not seek treatment in specialty substance use treatment clinics, often because of barriers such as long waiting lists and lack of transportation or childcare. One way to overcome these barriers is to offer AOUD treatment in primary care settings, where millions of Americans receive health care. Dr. Sarah Hunter, Dr. Allison Ober, and colleagues from the RAND Corporation recently showed that primary care facilities can provide AOUD treatment if staff training and funding for medication-assisted treatment (MAT) and ancillary services such as care coordination and psychosocial treatment are available. The research also showed that certain patient subgroups are more likely to use such treatment services. Dr. Ober says, “Publicly funded primary care organizations, with adequate support, can effectively deliver substance use treatment, thereby significantly expanding access to treatment in the United States.”
The researchers analyzed data from a large clinical trial testing AOUD treatment implementation in two clinics operated by a federally qualified health center that were serving low-income patients. Clinic staff were trained in AOUD screening and treatment, and the clinics implemented a collaborative care model where patients had access to a care coordinator and were offered behavioral treatment (BT) and MAT (i.e., extended-release naltrexone or buprenorphine/naloxone).
Primary Care Providers Support AOUD Treatment
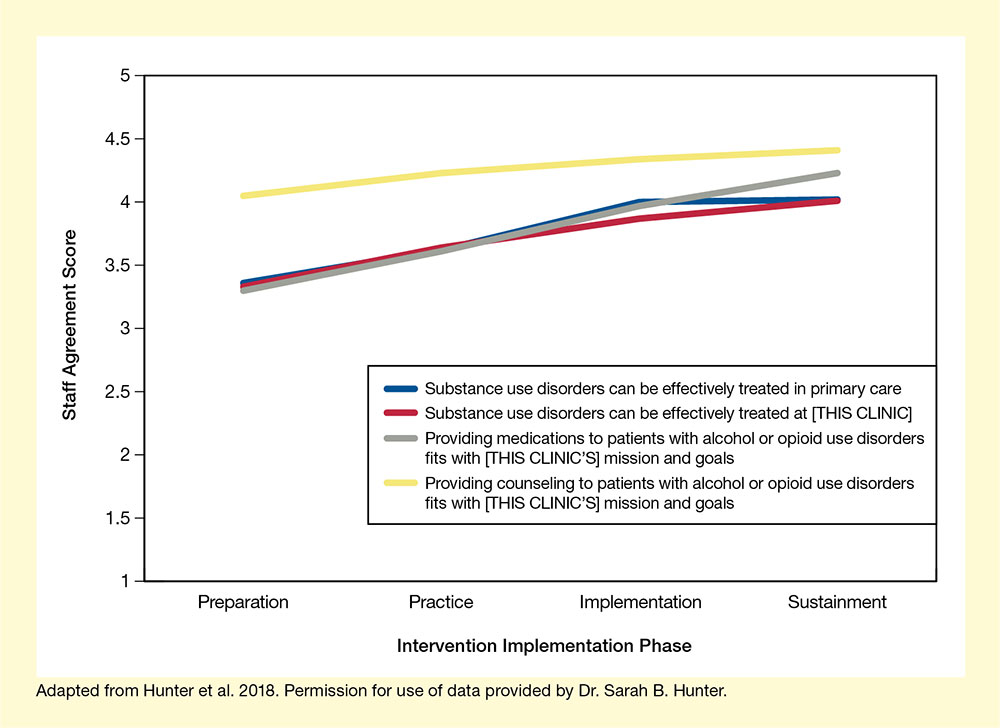
The RAND researchers’ two analyses looked at both the clinics and the patients to identify characteristics that influence whether AOUD treatment in primary care settings works. Dr. Hunter and colleagues examined the staff’s attitudes toward AOUD treatment throughout the trial and for 1 year afterwards (i.e., the sustainment period). Both clinic staff and leadership strongly supported the program (see Figure), and the number of patients receiving care coordination and BT for AOUD during the sustainment period increased significantly compared with the original trial. However, specific elements of the program—especially screening, collaborative care, and MAT—were modified during the sustainment period based on the available staff and funding. The staff were particularly concerned about reimbursement of MAT costs and considered this concern the greatest barrier to continued AOUD care.
Dr. Hunter concludes that the success of AOUD treatment in primary care settings will ultimately depend on the individual clinics’ capacity to provide ongoing staff training and services, which require stable sources of financial support. “In many instances, researchers find that organizations are not able to sustain evidence-based practices after the initial external support from the clinical study ends. Our finding suggests the particular importance of organizational readiness in building long-term support for the provision of substance use treatment in the primary care setting,” she says. Dr. Hunter adds, “More work is needed to determine the core elements of organizational readiness and the intensity of interventions needed to build capacities of nontraditional substance use care providers, like primary care, to identify and address substance use.”
AOUD Treatment in Primary Care Settings Reaches Specific Patient Subgroups
In the second analysis, Dr. Ober and colleagues examined which patients were most likely to begin AOUD treatment in the primary care clinics. Dr. Ober explains, “Understanding patient predictors of receiving treatment in primary care for an opioid or alcohol use disorder is a crucial first step toward designing programs that meet patients’ needs and ensuring that disparities are addressed.”
The analysis identified distinct characteristics of those initiating BT and MAT compared with those who did not initiate (see Table). Primary care patients with higher self-stigma around their substance use were more likely to initiate BT, while those who were homeless or had been arrested in the last 90 days were less likely. Female and older patients were more likely to initiate MAT. Also, patients who had already received BT were more likely to also initiate MAT and vice versa, suggesting that a collaborative care approach offering multiple services may improve the patients’ likelihood of receiving AOUD treatment. Dr. Ober says, “Successful treatment initiation starts with active linkage to treatment, and with the right intervention, patients attending primary care visits for problems other than substance use disorders are willing to initiate substance use disorder treatment in the primary care setting. Our study also suggests that a better understanding of gender and racial/ethnic differences and how to engage unstably housed individuals in care is needed.”
| BT | MAT |
|---|---|
|
Increased Likelihood of Initiating BT
|
Increased Likelihood of Initiating MAT
|
|
Reduced Likelihood of Initiating BT
|
Reduced Likelihood of Initiating MAT
|
Dr. Ober concludes that primary care settings can help expand treatment options for patients with AOUD. She states, “In the long term, studies will need to test multisystem collaborations so patients can be identified in multiple care settings and directed to receive treatment in the setting that best meets their needs.”
These studies were supported by NIDA grant DA034266.
- Text Description of Figure
-
The graph shows staff endorsement of four statements regarding AOUD treatment in primary care settings throughout an intervention implementation study. The horizontal x-axis shows the four implementation phases—preparation, practice, implementation, and sustainment. The vertical y-axis shows staff endorsement as indicated by a staff agreement score on a scale from 1 to 5. For the statement “Substance use disorders can be effectively treated in primary care” (blue curve), staff agreement scores were about 3.3 during the preparation phase, about 3.6 during the practice phase, about 4.0 during the implementation phase, and about 3.9 during the sustainment phase. For the statement “Substance use disorders can be effectively treated at [THIS CLINIC]” (red curve), staff agreement scores were about 3.3 during the preparation phase, about 3.6 during the practice phase, about 3.8 during the implementation phase, and about 3.9 during the sustainment phase. For the statement “Providing medications to patients with alcohol or opioid use disorders fits with [THIS CLINIC’S] mission and goals” (gray curve), staff agreement scores were about 3.3 during the preparation phase, about 3.6 during the practice phase, about 3.9 during the implementation phase, and about 4.2 during the sustainment phase. For the statement “Providing counseling to patients with alcohol or opioid use disorders fits with [THIS CLINIC’S] mission and goals” (yellow curve), staff agreement scores were about 4.1 during the preparation phase, about 4.3 during the practice phase, about 4.4 during the implementation phase, and about 4.4 during the sustainment phase.
Sources:
- Hunter, S.B., Ober, A.J., McCullough, C.M., et al. Sustaining alcohol and opioid use disorder treatment in primary care: A mixed methods study. Implementation Sci 13(1):83, 2018.
- Ober, A.J., Watkins, K.E., McCullough, C.M., et al. Patient predictors of substance use disorder treatment initiation in primary care. J Substance Abuse Treat 90:64-72, 2018.